
Information System for Screening and Automation of Document Management in Oncological Clinics
Authors Info & Affiliations
Abstract
Introduction:
Automation of business documentation workflow in medical practice substantially accelerates and improves the process and results in better service development.
Methods:
Efficient use of databases, data banks, and document-oriented storage (warehouses data), including dual-purpose databases, enables performing specific actions, such as adding records, introducing changes into them, performing an either ordinary or analytical search of data, as well as their efficient processing. With the focus on achieving interaction between the distributed and heterogeneous applications and the devices belonging to the independent organizations, the specialized medical client application has been developed, as a result of which the quantity and quality of information streams of data, which can be essential for effective treatment of patients with breast cancer, have increased.
Results:
The application has been developed, allowing automating the management of patient records, taking into account the needs of medical staff, especially in managing patients’ appointments and creating patient’s medical records in accordance with the international standards currently in force. This work is the basis for the smoother integration of medical records and genomics data to achieve better prevention, diagnosis, prediction, and treatment of breast cancer (oncology).
Conclusion:
Since relevant standards upgrade the functioning of health care information technology and the quality and safety of patient’s care, we have accomplished the global architectural scheme of the specific medical automation system through harmonizing the medical services specified by the HL7 international.
1. INTRODUCTION
Automation of business processes has long been firmly entrenched in our lives. It facilitates numerous human professional activities, including those involved in the medical industry, thus allowing to accelerate, simplify, and structure the performed work. The expansion of automating technical documentation can be realized through the introduction of automated control systems. In an oncology clinic, such systems can establish the efficient administration of the medical practice. At the same time, patients also require to receive objective treatment reports and diagnoses, with digital signatures of the treating physicians. The clinic management should ‘see’ their business as a whole, quickly identifying various problems and monitoring and stopping abuses. Automation of documenting medical practice accelerates and improves work processes significantly, which leads to better development of the services it provides. The use of databases and data banks, including those for dual purposes, makes it possible to perform specific actions, such as add records, make changes, perform a simple and analytical search of data, and effectively process them [1]. Nowadays, information technology allows the real turn of all documents into an electronic form in clinics so that the concerned doctor can find the necessary information within minutes.
Though some research describes a prototype of medical information and patient data processing system for an oncology clinic [2-4], in this paper, we report an automated system for managing the medical and administrative processes in the oncology clinic.
Methods of research: We used the following methods of research: system analysis, structural and functional approach, analysis of publications on the subject, comparison, generalization of cognitive and negative features of similar systems, and critical testing of the proposed development [5, 6].
The practical value of the carried-out work is that its results can be used to create an automated information system for the medical institution administration and doctors, including maintaining clinical information contained in the patient records.
2. MATERIALS AND METHODS
2.1. Information Technologies in Health Care System
Over the past five years, there has been a slight movement towards creating specialized automated systems for managing medical facilities, including patient records and electronic card management. However, it should also be noted that developing such systems is quite risky since the economic efficiency of their presence significantly dominates their costs, therefore, new developers are quite rare to appear in this area. Another significant obstacle to developing specialized automated health care systems is the lack of financial support for medical institutions, including clinics, as well as the need for a common strategy and understanding of the digitalization of document flow, which ensures the use of information technologies, making it possible to improve the quality of medical institutions in due time [7, 8]. One other significant disdvantage in the development of specialized automated systems is the lack of standardization of unstructured or poorly structured data, including ways to extract and process confidential data, such as patient diagnoses. Simultaneously, the national health care system encounters numerous challenges, such as increased patient requirements to meet the standards of service provided by the health care system, limited funding, frequent changes in the patients’ place of residence, etc. The application of specialized information systems, allowing to organize the management of medical clinics on the functional and innovative level, will significantly improve not only the quality of oncology treatment but also the level of medical services, which, in turn, will ensure the efficiency and cost-effectiveness of the use of available medical resources [9-14]. Information provided to the regional health departments, sanitary-epidemiological stations, and other medical institutions regarding epidemiological situation and the current state of morbidity is highly unsatisfactory, as is the availability of free beds in hospitals and the like.
Due to the lack of modern technology, software and telecommunications, such information is often incomplete or late, which does not allow management to quickly and professionally prevent possible threats, as well as to respond promptly to current problems that may arise in medical clinics [15-17]. Most medical information systems currently functioning in medical institutions are morally and physically outdated. Most of them were developed 10 - 20 years ago, and no one has maintained and improved them for a long time. What such systems allow is only automating the preparation of reporting forms.
Today on the Ukrainian market of medical information systems, there are about 15 developers [18, 19]. From the implemented developments, the following are worth mentioning: MedSistema, Siet, UkrMedSoft, Ther Dep. Polish (AVS), Russian (MeDialog). Turkish developers of medical information systems are also interested in the Ukrainian market, however, the cost of implementing their products is much higher than that of similar Ukrainian systems. Most systems are based on client-server architecture, which provides a limited number of functions, i.e., mainly the preparation of statistical reports and standard forms. Such systems maintain an electronic history but lack the function of digital signatures for recording the diagnosis in the patient’s electronic card, which is entered there by typing text or phrases from directories. This approach does not allow for further in-depth analytical analysis. The disadvantage of such systems is the need to contact the developers to make changes in the input and output forms. It is gratifying to see the appearance of domestic developers of the systems who support 3-level architecture. These systems are ‘Doctor Eleks’ and ‘EMCImed’, which are focused not only on the public but also on private medical institutions. They integrate an electronic patient card with numerous diagnostic equipment and data acquisition directly from laboratory analyzers. The entry of medical data into electronic history is based on the protocols developed by expert doctors [20-24]. Moreover, it opens ample opportunities for further comprehensive analysis of the data. These systems have a constructor for input and output reporting forms; they allow the exchange of document templates. The medical information system ‘Doctor Eleks’ deserves special attention. It was developed taking into account modern standards and principles of compatibility of medical information systems. The system is based on the concept of building medical examinations. The system meets all the information needs of the medical rehabilitation and diagnostic processes, research, educational and methodical work [25-27]. ‘Eleks’ (Lviv) started developing an information system back in 2000. The ‘Avalon system’ was the first development of the company, implemented in many medical institutions of the country. ‘Eleks’ was further developed as an oncology system for the University of Tampa (California, USA) and a large system for collecting statistics for the American market, using the HL7 international standard.
In the standard medical information system, an HL7 message verification mechanism must be installed to ensure the accuracy, legality, and completeness of medical information exchange. Based on an accurate string-matching algorithm, the HL7 message checking method can effectively increase the efficiency and stability of medical information exchange.
Based on the HL7 message analysis, an effective verification rule is established, and an SQL ABS string matching algorithm is proposed by combining the search skip algorithm and the fast search algorithm with the ABS algorithm. The algorithm achieves the maximum distance by calculating the distance between the skip value of the search algorithm and the fast search algorithm shift value, and then optimizing the order of the optimal matching sequence in the ABS algorithm, thereby reducing the number of matches and improving the algorithm performance. The experiments show that this method can effectively increase the efficiency of HL7 message checking and medical information exchange. In order to achieve interaction between distributed and heterogeneous applications and devices belonging to independent organizations, a client application is developed, resulting in an improved quantity and quality of information that may be relevant for the treatment of breast cancer patients. The application to automate the management of medical records is also developed to meet the needs of medical staff, especially in managing patients’ appointments and creating medical records according to the standards currently in use [28-30]. This work is the basis for integrating medical records and genomic data, which can lead to improved prevention, diagnosis, prognosis, and treatment of cancer (precise oncology) [31-33].
Relevant standards can improve the functioning of health information technologies and contribute to improving patient quality and safety [34]. The global architecture scheme has been implemented by harmonizing the medical services offered by HL7. The result of all innovations was the system ‘Doctor Eleks’, developed on the latest technologies, taking into account the experience and knowledge gained by specialists of the company during working on previous systems.
The Department of Health allows optimal input, storage, and analysis of not only basic patient data usually used in the registration, but also all medical records, such as complaints, anamneses and diseases, objective examination data, functional and laboratory diagnostics, anthropometry, as well as data on medical appointments and their implementation during their stay in the facility. The main component of patient data stored in the information system is an electronic medical record, which accumulates all information, i.e., data from medical examinations, anthropometric measurements, video control data, dynamic patient monitoring diaries, extracts and examination results from other clinics, multimedia data (X-rays, photo samples), and other essential data about the patient.
2.2. Main Aspects of the Medical Activity of the Oncology Clinic
In today’s environment, large enterprises and hospitals depend on information flows of data, and as a rule, these data are managed and processed through the database and bank server. Managing the flow of poorly structured patient clinical data is an archival task that requires more time for processing and responding to requests by systems for patient records. Taking this into consideration, we use some methods of analyzing the structured and unstructured data. To solve the above-described problems, we have proposed the development of an automated medical system for the oncology clinic that can easily handle the daily records of patient diagnoses. For this purpose, we used the symbiosis of databases for daily clinical records, thus eliminating a significant part of the routine work done by the medical clinic staff. The extraction and processing procedures will be applied to the agreed databases (normalized) and, later, converted into warehouses. By employing emergency data analysis methods and using both relational databases and repositories, we offer a methodology for building an automated medical oncology system [35, 36]. The data warehouse is based on an information database built by transforming the operational database. The data analyst can analyze the data and make decisions; it offers suggestions and predicts diseases using data and metadata. Based on data analysis methods, we also offer a clinical data warehouse model [37, 38]. The overall system is implemented in such a way that it effectively serves as a data warehouse for the medical information system.
Information and communication technologies used in the technological processes of prevention, treatment, diagnosis, and management of the medical clinic, are one of the main objectives of formalization and standardization in the health care system, which in turn requires the unification of service documents (including patient cards), basic terms and concepts, i.e., a unified approach to the treatment process. We can highlight the main aspects of information on the medical activity of the oncology clinic, i.e., technical, medical, technological, psychological, and pedagogical. The medical one involves the appropriate preparation of medical data and knowledge (formalization, unity of terminology, standardization), the creation of a user-friendly interface of the general structure of the information base in the form of a relational model and/or document-oriented model. The medical aspect also includes the construction of mathematical models of medical and biological processes (physiological and pathological), etc.
The technical aspect of the problem covers: 1) the development of theoretical models of data and knowledge representation for the solution of relevant medical issues and 2) specific hardware-software implementation of the information base based on the developed models. The technological aspect coordinates the developed technical automated system and a technological scheme of the medical and diagnostic processes (figuratively speaking, i.e., ‘a specific recipe for the implementation’ of the automated system in the medical and diagnostic process) [38]. And finally, the psychological and pedagogical aspects imply the appropriate training of medical personnel. The tasks to be solved with the help of computer technologies in medicine and healthcare are rather diverse. They differ both in purpose and content, as well as in directions and degree of use.
2.3. Screening Automated Medical Oncology Systems
Screening systems fall under the category of automated information medical oncological systems providing an effective solution to the urgent issue of collecting and processing information flows of data on the current state of the population health.
Screening systems are medical information systems at the level of therapeutic and preventive care in medical institutions (clinics). They are designed for pre-hospital preventive examination of population, clustering risk groups, and timely identification of patients needing specialist (doctor’s) assistance [39]. Screening is carried out based on the filled-in patient medical card or direct dialogue of the patient with an automated screening system deployed on a software and hardware complex with automated workplaces. Now we can formulate the tasks solved by such information systems at the level of outpatient institution (clinic), which are as follows 1) improvement of medical efficiency of preventive examinations in all pathology profiles (6 - 10 times) and 2) transition from formal reporting to accurate qualitative control of patients considering their health.
The system provides general health results of a particular patient or a team of people working in aggressive environments, and, accordingly, identifies negative causes in integral profiles directly related to the peculiarities of life of the team. It also helps to identify the disease at the early stages of implementation and to get an accurate assessment of the quality of treatment and rehabilitation measures. The most significant type of screening automated cancer systems is regular preventive examinations of the population [40]. Their main task is to identify patients in need of referral to specialized doctors and specialists at an early stage. Screening systems are designed for pre-hospital preventive examination of the population, the formation of risk groups, and identification of patients in need of specialist assistance [41, 42].
The value of such screening systems is that they consolidate all information flows and present them as a single system, capable of providing automation of various types of information analysis with subsequent management decisions. In accordance with the types of treatment and preventive care facilities, there are three software packages distinguished, i.e., the information systems ‘Inpatient’, ‘Clinic’ and ‘Emergency’. The initial information from these systems can be used to solve both local management tasks of the respective treatment and preventive care institution and top-level health care system tasks.
2.4. Mathematical Apparatus to Support Medical Decision-Making in the Treatment of Oncology Patients
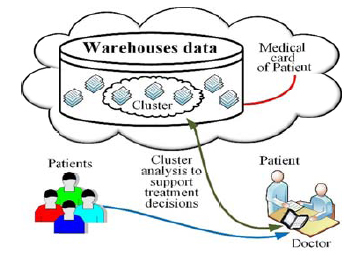
For correct decision-making regarding the diagnosis and treatment of the oncology patient, after preliminary examination of the patient, the doctor, if necessary, can refer to the data storage of all patient histories to find a similar diagnosis, which can be located either on the local server or in the cloud services. Following the procedure, the doctor predetermines the characteristics for the cluster, which saves the histories of those patients whose age range, diagnosis, and concomitant diseases are most similar to the characteristics of the patient under treatment. Based on the accumulated repository data, the system analyses accessible diagnoses for similarity and offers relevant patient cards for detailed analysis, followed by a treatment algorithm. The attending physician can either agree to them or change the search criteria for related cancer histories and seek a more relevant search result of the treatment algorithm. This approach provides a short-term opportunity to compare the cards of oncology treated cases with positive treatment indicators with the medical card of the patient admitted for treatment; this approach, in turn, provides a correct diagnosis and helps to find the best treatment algorithm in the shortest possible time (Fig. 1).
Cluster analysis (clustering) is a technology that allows you to distribute incoming data into classes, i.e., groups of similar sample instances or clusters – compact areas of grouping sample instances in the space of features. The initial information for clustering is a sample of observations, where n is the number of values of sample instances n = 1, 2, ..., n, m is the number of features characterizing sample instances m = 1, 2, ..., m.
To provide cluster analysis, we form a set of n-objects (cancer patient cards), each of which is described with m-symptoms or comorbidities, and set in the form of an input data matrix X, or standardized data Z, n*m. Thus, we will get a matrix of observations with input information for detailed analysis and comparison with the base record, each row of which n are the values of features m of one of the S objects of clustering.

3. RESULTS AND DISCUSSION
3.1. Application of Case-based Reasoning Convergence for Solving Medical Problems
In medicine, case-based reasoning (i.e., reasoning based on medical precedents) is a new effective methodology adapted from artificial intelligence. It enables the hybridization of reasoning methods and machine learning methods to solve medical problems based on previous experience of diagnosing patients and treatment courses in the form of patient’s case studies. Consider the construction of a signature for a typical case in the medical field for disease prediction. Let’s introduce the sequences of controlled medical parameters (cp- parameters), uncontrolled medical parameters (ucp- parameters), disturbing medical parameters (dcp - parameters) and resulting medical parameters (op - parameters).
The initial case matrix of medical indicators will look like:

Since most of the encased parameters will have constraints imposed on them, it would be logical to proceed to the template (X,D,C) where X is the set of variables (parameters), D is the domain of values of medical parameters, C is the set of constraints imposed on medical parameters. The course of patient treatment will occur in a number of its condition’s states Cure.Statei ,  . Each medical parameter from the initial signature matrix
. Each medical parameter from the initial signature matrix  , where
, where  or
or  in accordance for
in accordance for  will take the appropriate values from the regulated domains of controlled or uncontrolled parameters change, respectively. Let’s conceptualize the main stages of functioning of the proposed technique for the development of the system based on the medical cases database.
will take the appropriate values from the regulated domains of controlled or uncontrolled parameters change, respectively. Let’s conceptualize the main stages of functioning of the proposed technique for the development of the system based on the medical cases database.
3.1.1. Extraction
Extraction of existing medical cases is similar in content to the body of the case-request method for a course of treatment based on convergent methods and techniques. The strategy of learning from the cases is performed at the initial level of implementation.
3.1.2. Use of the Solutions
Solutions ( i.e., previously successful patient treatment courses ) are based on a set of cases of successful patient treatment, which become the basis for creating a new solution (in our case, a treatment regimen) relevant to a request done for a particular new patient, with some additions, depending on the situation.
The solution will be produced, for example, by sequential comparison based on the convergence technique in the imposed constraints systems 
The required minimal evaluation will be as follows 
The result for the basic sets of variables (medical symptoms) will be as follows  .
.
3.1.3. Modification of the Decision
Modification of the decision comes in the form of the recommended course of treatment obtained as a result of the execution of the case request, with the adjustments made in accordance with the level of satisfaction of the initial parameters constraints or level of relevance:, 
3.1.4. Cataloguing of the Medical Decision
Cataloguing the medical decision means inserting a new course of treatment. According to the conclusions made at Step 3, the insertion of a relevant case into the database of medical cases will follow, thus adding new knowledge to the knowledge base with consistency testing: 
3.2. Practical Implementation of a Screening Information System for Automated Document Processing in an Oncology Clinic
Since the number of clinical guidelines and rules for effective patient management with active oncology diagnostics is steadily growing at the clinic level, there is an increasing need for automated medical screening systems to register patients and support treatment decisions.
With this in view, in this paper, we present a general knowledge management system for oncological diseases intended for supporting effective decision-making and intelligent diagnostics [43-46]. While collaborating, clinicians can establish and use different rules regarding knowledge and experience, afterwards summarizing them and applying them to patient data collected in the personal medical record [47-49]. The generated knowledge is formulated as an unstructured text and is returned to clinicians to inform them with adequate information, on the one hand, and to help them improve communication with patients, on the other. For these purposes, we have developed an information screening medical oncology system 'Medical Oncology Center.' 'Medical Oncology Center' is a sufficiently developed triggered system designed to be used by other users, guests, administrators, and doctors with the system. The same is true for access to personal information in the system. The system can be used by several access groups to log files (Fig. 2). Several groups can access the system to log files.
Now we will consider the algorithm that the automated medical system follows while adding a message to the patient history, concerning different user groups and access groups (Fig. 3).
Therefore, based on the system adaptability to any of the above-defined groups of users, we conclude that the system is usable in different ways; i.e., when trying to display a patient’s medical history with no records, the system will return the corresponding message which, in its turn, will disappear as soon as at least one new entry is added. Simultaneously, all available records from the patient’s medical history are delivered/returned. If the existing records are deleted as a part of the ongoing process, the system also reports their absence. Fig. (4) highlights the algorithm of the data trigger process.



When observing any automated medical system, one finds out the significant feature they all have in common, i.e., any action performed by a user is to be followed by the message informing about the success or failure of the carried-out operation. Otherwise, the user may accidentally enter false data without noticing the mistake made. Consequently, after every action concerning data changing, especially personal data, either an approving or rejecting message appears (Fig. 5).

If a user (patient) is previously registered, or some wrong actions have been performed, the automated medical system issues a relevant message that reads, e.g., (Fig. 6):
- Password is less than 8 characters;
- E-mail already used by another user;
- Empty fields
The system warns about users' errors and prevents creating a new user's profile with invalid input data. Once users have entered the information correctly, new profiles are to be created automatically. Simultaneously, new owners are automatically redirected to their respective profiles. Other types of data limitations spotted by the automated medical system, ‘Medical Oncology Center’ have been mentioned in Table 1.
In the present-day world, the internet is accessible on different types of devices, therefore, oncologists, administrators, other clinic personnel, and patients use it all the time. With this in mind, we consider another characteristic of the system, i.e., its adaptability. The adaptability of a screening medical and oncological system plays an essential role in the interaction with the system, as it determines the availability of the system and its ease of use on different devices. Expecting users to use one type of platform for interaction with the system in modern realities is a bad idea. Therefore, we consider the adaptability of the system ‘Medical Oncology Center’ in different conditions and states (Fig. 7).

| No. | Data Type Name | Limitation |
|---|---|---|
| 1 | Name of the department | Cannot be empty at the time of the creation Cannot exceed 100 characters |
| 2 | Id posts in medical history | Cannot be empty at the time of the creation |
| 3 | Post | Cannot be longer than 1000 characters |
| 4 | User name | Cannot be more than 50 characters Cannot be empty at creation |
| 5 | User's name | Cannot be more than 50 characters |
| 6 | Last name | Cannot be more than 50 characters |
| 7 | Address | Cannot be longer than 300 characters |
| 8 | Must match the format Cannot be empty at the time of the creation Must be unique |
|
| 9 | Phone | Must match the format Cannot be more than 15 characters |
| 10 | Home phone | Must match the format Cannot be more than 15 characters |
| 11 | Password | At least 8 characters |
Fig. (7) visualizes the adaptability of the system ‘Medical Oncology Center’ to different conditions and user gadgets. The application of the robotic system for the expansion of the screen needs 1000 px.
Fig. (8) highlights the system performance quality on different user mobile devices (tablets, smartphones, car panels, etc.), i.e, its adaptability to different resolutions.


CONCLUSION
While developing a screening automated medical documentation processing system, the business-documentation workflow of the oncology clinic was automated, which substantially accelerates and improves the interaction of the medical staff in the workplace and results in better service development. The efficient use of databases, data banks, and document-oriented storage (warehouses data), including dual-purpose databases, enables qualitative and quick performing specific actions, namely adding records, introducing changes into them, performing both the ordinary and analytical search of data, as well as their efficient processing, in turn, ensures quality managerial (treatment) decisions. With the focus on achieving interaction between the distributed and heterogeneous applications and the devices belonging to the independent organizations, the specialized medical client application has been developed; as a result, both the quantity and quality of the information streams of the data essential for effective treatment of patients with breast cancer have increased. The developed application enables automating the management of patient records, taking into account the needs of medical staff, especially in managing patients’ appointments and creating patient’s medical records in accordance with the international standards currently in force. This work is the basis for the smoother integration of medical records and genomics data to achieve better prevention, diagnosis, prediction, and treatment of breast cancer (oncology). Since relevant standards upgrade the functioning of health care information technology and the quality and safety of patient’s care, we have accomplished the global architectural scheme of the specific medical automation system through harmonizing the medical services specified by the HL7 international that ensures the system’s scalability in the future.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
Medical system on the basis of the experimental data is in the testing phase.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

