
Genotypic-phenotypic Profiling and Statistical Modeling of the icaA Biofilm Marker in Multidrug-resistant Staphylococcus on Iraqi Currency
Authors Info & Affiliations
Abstract
Introduction
Paper money has served as a fomite and vector for centuries, potentially harboring pathogenic microorganisms due to contamination with nosocomial infections, such as biofilm-forming, multidrug-resistant bacteria. This study was conducted to examine environmental contamination of Iraqi current currency notes with bacteria, biofilm-forming genes, and antimicrobial-resistant profiles.
Methods
In this cross-sectional study, 32 Iraqi currency notes were obtained from six commercial sectors (October 2024–February 2025). Bacterial identification was performed using standard methods and the VITEK-2 automated system. Antimicrobial susceptibility testing was performed using the Kirby-Bauer disk diffusion method (CLSI 2024 criteria). PCR amplification was used to detect the icaA gene. Statistical analysis was performed using the chi-square and Fisher's exact tests (p-value < 0.05).
Results
All 32 currency notes (100%) were positive for contamination, yielding a total of 50 bacterial isolates. Overall, Staphylococcus species were the most frequently isolated organism (n = 29, 58%), with S. epidermidis representing the most common isolate (n = 19, 38%). High rates of resistance were recorded for oxacillin (86.2%) and erythromycin (79.3%). In terms of multi-drug resistance, fifteen (51.7%) isolates were multi-drug-resistant (MDR). The icaA gene was present in 18 of 29 (62.1%) Staphylococcus isolates and was significantly associated with robust biofilm production (p-value < 0.001).
Discussion
The presence of multidrug resistance and the biofilm-associated gene IcaA among the isolates indicated an apparent public health risk. This reflects the highly active, community-wide circulation of antimicrobial-resistant and highly persistent pathogens that survive both antibiotics and host defenses during everyday interactions.
Conclusion
The significant burden of these high-risk bacteria on Iraqi currency underscores the urgent need to raise hygiene levels at the community level and to develop effective control strategies to prevent money from serving as a vehicle for pathogen transmission.
1. INTRODUCTION
Paper money is probably the most commonly used object in human civilization, serving as the dominant form of economic exchange across various ethnic and geographic territories. Currency is everywhere and can serve as an ideal medium for the acquisition, persistence, and transmission of infectious agents. The role of contaminated currency as a potential transmitter of pathogenic microorganisms in developing countries, where cashless payment systems remain limited and dissuade adoption [1]. Related epidemiologic reports also indicate that banknotes/coins may carry viable bacteria over a long period, and the rates of contamination are not low (ranging from 69 to 100%, varying with different currencies all over the world) [2, 3].
The public health importance of currency contamination was further emphasized by the COVID-19 pandemic, which revealed that fomite transmission of causative agents, emphasizing the prominence of those circulated objects [ 4 ]. Coin and paper currency notes have high water-holding properties, contain a natural source of carbon for bacteria to grow on, and are in people's hands, which come into contact with a change given back by sellers [ 5 ]. This is especially important in commercial market environments, restaurants, and so on, where currency transactions occur during food preparation and handling of animal products, which can harbor pathogenic microorganisms [ 6 ].
Modern research has revealed varying bacterial populations on notes that include both commensal and pathogenic species. A study of the Thai banknotes and coins using matrix-assisted laser desorption/ionization time-of- flight mass spectrometry (MALDI-TOF MS) showed that 93.33% of the banknotes and 30.00% of the coins were contaminated with bacteria, while fish shops presented the highest contamination [7]. Studies carried out more recently on the denomination of currency notes in Pakistan showed frequent occurrence of pathogenic bacteria and presented a potential threat to public health [8]. These results are in line with those of previous studies carried out worldwide, and confirm that currency contamination is a global issue that warrants continuous monitoring and intervention. Among the bacteria frequently encountered on currency notes, staphylococci are of special concern because they have the potential to become pathogenic, acquire antimicrobial resistance, and form biofilms [9]. Staphylococcus aureus and CoNS, such as S. epidermidis, are commonly isolated from banknotes, and the species have been implicated in healthcare-associated infections, skin and soft tissue infections, and invasive diseases among immunocompromised patients [10]. These organisms’ ability to persist on inanimate surfaces for prolonged periods, along with the facility of their horizontal gene transfer, may make them excellent candidates for inter- and intra-community spreading antimicrobial resistance determinants [11].
Bacterial biofilm formation is an important virulence mechanism that promotes pathogen survival, antimicrobial resistance, and persistence in healthcare and community environments [12]. Biofilms are composed of organized microbial consortia encapsulated by a self-generated extracellular polymeric matrix for resistance to environmental conditions, host immune defenses, and antimicrobials [13]. Biofilm formation in Staphylococcus species is mostly due to the intercellular adhesion (ica) operon genes encoding for the synthesis of polysaccharide intercellular adhesin (PIA), including icaA, icaB, icaC, and icaD [14]. Specifically, the icaA gene, which encodes N-acetylglucosaminyltransferase, is involved in early biofilm development and has been reported as an important molecular marker for biofilm-forming ability [15].
Recent molecular epidemiological investigations indicated a significant relationship between the presence of ica genes and biofilm formation in clinical Staphylococcus isolates. On the other hand, based on a systematic examination of MRSA strains isolated from burn patients, the icaA gene was found to be the most common biofilm-associated gene detected in most biofilm-positive isolates [16]. Studies of clinical isolates of S. aureus from hospitalized patients indeed confirmed the fundamental contribution made by the icaADBC operon to biofilm formation, with relevant consequences on treatment and control of infections [17]. These results emphasise the contribution of biofilm-associated genes in the pathogenicity of Staphylococcus isolates from nonclinical sources.
The proliferation and spread of AMR among currency note-associated bacteria is an emerging public health issue, especially in countries with high antibiotic use and poor infection control practices [18]. The World Health Organisation [19] has named a number of multi-drug-resistant organisms in their 2024 Bacterial Priority Pathogens List as posing serious health threats at the global level, including fluoroquinolone-resistant Salmonella Typhi and Shigella species, vancomycin-resistant Enterococcus faecium, and carbapenem-resistant Pseudomonas aeruginosa. Circulation of currency so contaminated with these organisms could be a vehicle for community-acquired antimicrobial resistance, especially in the healthcare environment, where money is exchanged near patients.
MDR (multidrug resistance; resistance to three or more classes of antimicrobial agents) is a growing concern among bacterial isolates from environmental broths, such as currency notes and others [20]. Mechanisms of MDR development include the acquisition of resistance genes by horizontal gene transfer, chromosomal mutations targeting drug targets, or the overexpression of efflux pumps that promote the active removal of antimicrobial substances from cells [21]. In biofilms, resistance is further increased by reduced drug penetration and the development of oxygen- and nutrient-gradients, which foster persister cell formation and the exchange of resistant determinants between bacterial species [22].
The molecular identification of antimicrobial resistance genes and biofilm-related factors has become increasingly important for elucidating the epidemiology and clinical relevance of bacterial contamination in environmental specimens [23]. The PCR techniques are known for being fast, sensitive, and specific in detecting the virulence and resistance genetic markers, which would permit an extensive characterization of bacterial populations from banknotes [24]. These types of samples have recently concluded development for multiplex screening with molecular diagnostics able to detect different resistance genes and virulence factors at the same time, obtaining, as a consequence, more detailed information regarding genetic similarity of isolates obtained from environmental sources and their pathogenic potential [25].
The Iraqi health care setting is characterized by major problems of antimicrobial resistance, hospital-acquired infections, and limited infection control and surveillance resources [26]. The continuous reconstruction of the country, along with high urbanization density in cities and heavy trading, leads to the generation of favourable background circumstances for circulating contaminated money and spreading microorganisms [27]. Previous reports on currency contamination in Iraq have shown mixed populations of bacteria with differential antibiotic susceptibility and limited molecular epitope profiling of biofilm-associated genes [28, 29].
To the best of our knowledge, the present work bridges important gaps in the information about bacterial contamination of Iraqi paper currency in relation to molecular epidemiology concerning both biofilm formation and antibiotic resistance. This study employs the advantage of a genotypic-phenotypic profiling approach, which allows the analysis of genetic susceptibility profiles, including the presence of the icaA gene as well as their phenotypes (biofilm-forming capacity and interaction with antimicrobials). Such a dual approach offers a more detailed insight into the virulence parameters and clinical relevance of the bacterial isolates. Combining the identified genotypic marker (icaA) with its phenotypic expression of biofilm formation might allow us to more accurately evaluate the public health risk associated with these currency-seeding bacteria. In addition, this study includes the statistical modeling of icaA as a biofilm marker that can be used to provide a quantitative measure of its relationship with biofilm production and multidrug resistance.
2. MATERIALS AND METHODS
2.1. Study Design and Setting
This cross-sectional molecular epidemiological study was conducted from October 2024 to February 2025 in Iraq, focusing on the bacterial contamination of paper currency notes in active circulation. The overall methodology is summarized in the flowchart presented in Fig. (1). The study was designed to investigate the prevalence, diversity, and molecular characteristics of bacterial populations associated with Iraqi currency, with particular emphasis on biofilm formation genes and antimicrobial resistance patterns. All laboratory analyses were performed at the Microbiology Laboratory of the University of Alkafeel, Najaf, Iraq, following standard biosafety protocols and quality assurance procedures.
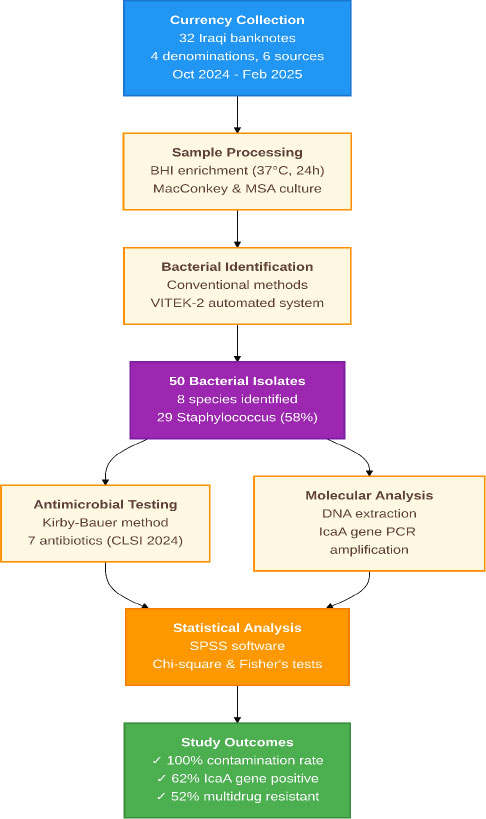
Methodology flowchart.
2.2. Sample Size Calculation and Justification
The sample size was calculated based on the expected prevalence of bacterial contamination in currency notes, estimated at 80% based on previous international studies [30, 31]. Using a margin of error of ±10%, a confidence level of 95%, and accounting for potential losses during processing, the minimum required sample size was determined to be 62 currency notes. However, due to logistical constraints and the exploratory nature of this pilot study, a convenience sample of 32 currency notes was collected, providing adequate power (>80%) for detecting large effect sizes in contamination rates between different currency denominations and sources.
2.3. Currency Note Collection and Sampling Strategy
Currency notes were collected using a systematic sampling approach designed to represent diverse commercial environments and currency denominations commonly circulated in Iraq [32, 33]. The sampling frame included six distinct commercial sources: fish vendors, vegetable sellers, cafeterias, butchers, taxi drivers, and gas station workers. These sources were selected based on their high frequency of currency handling, diverse customer populations, and varying levels of hygiene practices, providing a representative sample of currency contamination patterns in Iraqi commercial settings.
Four currency denominations were included in the study: 250, 500, 1000, and 5000 Iraqi dinars, representing the most commonly circulated paper notes in the Iraqi monetary system. Six notes of each denomination were collected from each source category, resulting in a total sample size of 32 currency notes (4 denominations × 6 notes per denomination, with 2 additional notes for quality control purposes). The collection was distributed across different geographic areas within Iraq to minimize location-specific bias and enhance the generalizability of findings.
Currency notes were collected through direct purchase transactions conducted by trained research personnel, ensuring that the notes had been in active circulation and represented authentic contamination patterns. Each note was immediately placed in a sterile plastic bag using aseptic techniques, labeled with a unique identifier indicating the collection source, denomination, date, and time of collection. The samples were transported to the laboratory under cold storage conditions (4°C) within 2 hours of collection to preserve bacterial viability and prevent overgrowth of environmental contaminants.
2.4. Bacterial Isolation and Identification
The bacterial isolation protocol was adapted from established methods for environmental sampling, with modifications to optimize recovery from currency note surfaces [34]. Each currency note was processed individually to prevent cross-contamination and ensure accurate attribution of bacterial isolates to specific samples. The entire surface of each note was systematically swabbed using sterile cotton swabs moistened with sterile phosphate-buffered saline (PBS, pH 7.4), ensuring comprehensive coverage of both sides of the currency.
The swab samples were immediately suspended in 5 mL of brain heart infusion (BHI) broth (Oxoid, UK) and incubated aerobically at 37°C for 24 hours to allow bacterial multiplication and recovery of potentially stressed organisms. Following enrichment, 100 μL of the BHI culture was plated onto MacConkey agar (Oxoid, UK) for the isolation of gram-negative bacteria and mannitol salt agar (Oxoid, UK) for the selective isolation of Staphylococcus species. All culture plates were incubated aerobically at 37°C for 24-48 hours, with daily examination for bacterial growth and colony morphology assessment.
Bacterial colonies displaying distinct morphological characteristics were selected for further identification and characterization. Each morphologically distinct colony type was subcultured onto blood agar (Oxoid, UK) to obtain pure cultures and assess hemolytic activity. Gram staining was performed on all isolates using standard protocols, followed by catalase and oxidase testing to differentiate between major bacterial groups. Preliminary identification was based on colony morphology, Gram stain characteristics, and basic biochemical reactions.
Definitive bacterial identification was performed using the VITEK-2 automated microbiology system (bioMérieux, France) with GN-ID cards for gram-negative bacteria and GP-ID cards for gram-positive bacteria. This system was selected for its high accuracy, rapid turnaround time, and extensive database of clinically relevant microorganisms, providing standardized and reproducible species-level identification. The VITEK-2 system utilizes 47 biochemical tests and provides species-level identification with confidence levels ranging from 85% to 99%. Only isolates with identification confidence levels ≥95% were included in the final analysis to ensure accuracy and reliability of species determination.
2.5. Antimicrobial Susceptibility Testing
Antimicrobial susceptibility testing was performed using the Kirby-Bauer disk diffusion method according to Clinical and Laboratory Standards Institute (CLSI) 2024 guidelines [35]. The antibiotic panel was selected based on clinical relevance, resistance surveillance priorities, and availability in the Iraqi healthcare system. For Staphylococcus isolates, seven antibiotics representing different classes were tested: tigecycline (15 μg), linezolid (30 μg), gentamicin (10 μg), ciprofloxacin (5 μg), clinda>mycin (2 μg), erythromycin (15 μg), and oxacillin (1 μg).
Bacterial suspensions equivalent to 0.5 McFarland standard were prepared in sterile saline and inoculated onto Mueller-Hinton agar plates (Oxoid, UK) using sterile cotton swabs to ensure confluent growth. Antibiotic disks (Oxoid, UK) were placed on the inoculated plates using sterile forceps, with appropriate spacing to prevent overlapping of inhibition zones. The plates were incubated aerobically at 37°C for 18-24 hours before measuring the zone diameter.
Inhibition zone diameters were measured to the nearest millimeter using digital calipers, and results were interpreted according to CLSI 2024 breakpoints for each antibiotic-organism combination. Quality control was performed using Staphylococcus aureus ATCC 25923 and Escherichia coli ATCC 25922 reference strains to ensure the accuracy and reproducibility of susceptibility testing results. MDR was defined as resistance to three or more classes of antimicrobial agents, following established epidemiological definitions [36].
2.6. Molecular Detection of the IcaA Gene
DNA extraction was performed using the Wizard Genomic DNA Purification Kit (Promega, USA) according to the manufacturer's instructions, with modifications for gram-positive bacteria. Bacterial cells from overnight cultures were harvested by centrifugation, resuspended in lysis buffer containing lysozyme (20 mg/mL), and incubated at 37°C for 30 minutes to facilitate cell wall digestion. The subsequent extraction steps followed the standard protocol, including protein precipitation, DNA precipitation, and final resuspension in nuclease-free water.
The quality and quantity of extracted DNA were assessed using spectrophotometry (NanoDrop 2000, Thermo Scientific, USA) and agarose gel electrophoresis. DNA samples with A260/A280 ratios between 1.8 and 2.0 and concentrations ≥50 ng/μL were considered suitable for PCR amplification. All DNA samples were stored at -20°C until use, with working aliquots prepared to minimize the number of freeze-thaw cycles.
PCR amplification of the icaA gene was performed using specific primers designed to amplify a 188-bp fragment of the gene encoding N-acetylglucosaminyl>transferase. The primer sequences were: forward primer 5'-ACACTTGCTGGCGCAGTCAA-3' and reverse primer 5'-TCTGGAACCAACATCCAACA-3' (Alpha DNA, USA). The PCR reaction mixture (25 μL total volume) consisted of 12.5 μL of 2× PCR Master Mix (Ampliqon, Denmark), 1 μL each of forward and reverse primers (10 pmol/μL), 2 μL of template DNA (approximately 100 ng), and 10.5 μL of nuclease-free water.
The PCR amplification was performed using a thermal cycler (Bio-Rad, USA) with the following conditions: initial denaturation at 95°C for 5 minutes, followed by 35 cycles of denaturation at 95°C for 30 seconds, annealing at 55°C for 30 seconds, and extension at 72°C for 30 seconds, with a final extension at 72°C for 7 minutes. Positive and negative controls were included in each PCR run to ensure specificity and detect potential contamination. Staphylococcus epidermidis ATCC 35984, a known icaA-positive strain, was used as the positive control, while nuclease-free water was used as the negative control.
PCR products were analyzed by electrophoresis on 1.5% agarose gels (SinaClon, Iran) containing ethidium bromide (0.5 μg/mL) in 1× TAE buffer at 100V for 45 minutes. A 100-bp DNA ladder (SinaClon, Iran) was used as a molecular weight marker to confirm the expected product size. Gels were visualized under UV transillumination (Cleaver Scientific, UK) and photographed using a gel documentation system. The presence of an 188-bp band was considered indicative of icaA gene positivity.
2.7. Biofilm Formation Assay
The biofilm formation ability of the Staphylococcus isolates was assessed by a microtiter plate assay, followed by crystal violet staining. In short, overnight bacterial cultures were grown in Tryptic Soy Broth (TSB) containing 1% glucose. The cultures were subsequently diluted 1:100 in fresh TSB, and 200 μL aliquots were dispensed into the wells of polystyrene microtiter plates with flat bottom (96-wells; Thermo, Waltham, MA, USA). Wells were subsequently washed three times with sterile phosphate-buffered saline 24 hours post-incubation at 37°C to remove non-adherent cells. The adherent biofilms were fixed with methanol, stained with 0.1% crystal violet for 15 minutes, and the bound dye was solubilized with 33% glacial acetic acid. The optical density was measured at 590 nm (OD590) using a microplate reader. The cutoff OD (ODc) for determining biofilm production was established by calculating the mean OD of the negative control wells (containing only TSB) plus three times the standard deviation. Isolates were classified as: strong biofilm formers (OD590 > 4×ODc), moderate biofilm formers (2×ODc < OD590 ≤ 4×ODc), weak biofilm formers (ODc < OD590 ≤ 2×ODc), or non-biofilm formers (OD590 ≤ ODc). All assays were performed in triplicate and repeated on at least two separate occasions.
2.8. Statistical Analysis
Statistical analysis was performed using SPSS version 29.0 (IBM Corporation, USA). Categorical data were presented as frequencies and percentages with 95% confidence intervals, and continuous data as means ± standard deviations. Associations between categorical variables were analyzed using Pearson's chi-square test or Fisher's exact test when expected cell counts were less than 5. Multivariable logistic regression was performed to identify independent predictors, with backward elimination and a significance threshold of p-value < 0.05. All statistical tests were two-tailed, with statistical significance defined as p-value < 0.05. This included the statistical modeling of the icaA biofilm marker, where logistic regression was used to quantify the association between the presence of the icaA gene (genotype) and the phenotypic expression of biofilm formation and antimicrobial resistance, thereby integrating the genotypic-phenotypic profiling approach described above.
3. RESULTS
3.1. Sample Characteristics and Bacterial Contamination Patterns
The study successfully collected and analyzed 32 Iraqi paper currency notes, representing four denominations (250, 500, 1000, and 5000 dinars), from six distinct commercial sources over a period of five months (Table 1). All currency notes (100%) demonstrated bacterial contamination, confirming the universal presence of microorganisms on circulating Iraqi currency. The contamination was evident through visible bacterial growth on selective media within 24-48 hours of incubation, indicating the presence of viable and metabolically active bacterial populations.
| Characteristic | n | % | 95% CI |
|---|---|---|---|
| Currency denomination | |||
| 250 dinars | 8 | 25.0 | 11.5-43.4 |
| 500 dinars | 8 | 25.0 | 11.5-43.4 |
| 1000 dinars | 8 | 25.0 | 11.5-43.4 |
| 5000 dinars | 8 | 25.0 | 11.5-43.4 |
| Collection source | |||
| Fish vendors | 6 | 18.8 | 7.2-36.4 |
| Vegetable sellers | 6 | 18.8 | 7.2-36.4 |
| Cafeteria | 4 | 12.5 | 3.5-29.0 |
| Butchers | 6 | 18.8 | 7.2-36.4 |
| Taxi drivers | 5 | 15.6 | 5.3-32.8 |
| Gas station workers | 5 | 15.6 | 5.3-32.8 |
| Study period | |||
| October 2024 | 8 | 25.0 | 11.5-43.4 |
| November 2024 | 7 | 21.9 | 9.3-40.0 |
| December 2024 | 6 | 18.8 | 7.2-36.4 |
| January 2025 | 6 | 18.8 | 7.2-36.4 |
| February 2025 | 5 | 15.6 | 5.3-32.8 |
| Physical condition | |||
| Good | 18 | 56.3 | 37.7-73.6 |
| Fair | 10 | 31.3 | 16.1-50.0 |
| Poor | 4 | 12.5 | 3.5-29.0 |
| Total currency notes | 32 | 100.0 | - |
| Total bacterial isolates | 50 | - | - |
| Overall contamination rate | 32 | 100.0 | 89.1-100.0 |
Note: CI: Confidence interval. Data presented as n (%) unless otherwise specified.
The distribution of bacterial contamination varied significantly across currency denominations (χ2 = 12.47, p-value = 0.006). The 1000-dinar notes exhibited the highest bacterial burden, with an average of 2.3 ± 0.8 distinct bacterial species per note, followed by 5000-dinar notes (1.9 ± 0.6 species per note), 500-dinar notes (1.7 ± 0.5 species per note), and 250-dinar notes (1.4 ± 0.4 species per note). This pattern likely reflects the frequency of circulation and handling, with 1000-dinar notes being the most commonly used denomination for daily transactions in Iraqi commercial settings.
3.2. Bacterial Species Identification and Distribution
A total of 50 bacterial isolates were recovered from the 32 currency notes, representing eight distinct bacterial species confirmed through VITEK-2 automated identification (Fig. 2 and Table 2). The bacterial population was dominated by gram-positive cocci, particularly Staphylococcus species, which accounted for 29 isolates (58% of the total). Among the Staphylococcus isolates, S. epidermidis was the most prevalent species (n = 19, 38% of total isolates), followed by S. aureus (n = 5, 10%), S. pseudintermedius (n = 3, 6%), and S. lentus (n = 2, 4%).
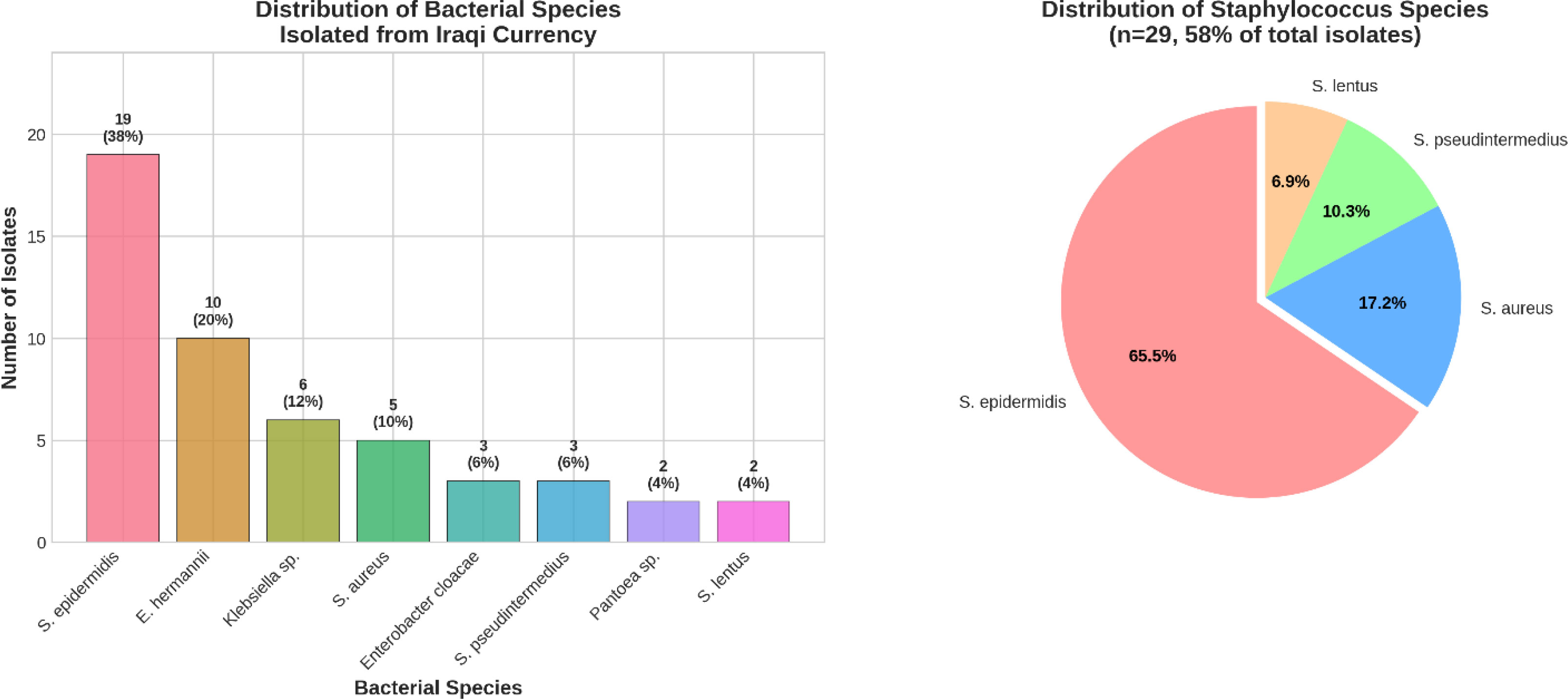
A) Bacterial species distribution and B) Staphylococcus species distribution.
| Bacterial Species | n | % of Total | 95% CI | Gram Stain | VITEK-2 Confidence (%) |
|---|---|---|---|---|---|
| Gram-positive bacteria | |||||
| Staphylococcus epidermidis | 19 | 38.0 | 24.7-52.8 | Positive | 97.2 ± 1.8 |
| Staphylococcus aureus | 5 | 10.0 | 3.3-21.8 | Positive | 98.4 ± 1.2 |
| Staphylococcus pseudintermedius | 3 | 6.0 | 1.3-16.5 | Positive | 96.7 ± 2.1 |
| Staphylococcus lentus | 2 | 4.0 | 0.5-13.5 | Positive | 95.5 ± 0.7 |
| Subtotal Gram-positive | 29 | 58.0 | 43.2-71.8 | ||
| Gram-negative bacteria | |||||
| Enterobacter hermannii | 10 | 20.0 | 10.0-33.7 | Negative | 97.8 ± 1.5 |
| Klebsiella pneumoniae | 6 | 12.0 | 4.5-24.3 | Negative | 98.1 ± 1.3 |
| Enterobacter cloacae | 3 | 6.0 | 1.3-16.5 | Negative | 96.3 ± 1.9 |
| Pantoea species | 2 | 4.0 | 0.5-13.5 | Negative | 95.0 ± 1.4 |
| Subtotal Gram-negative | 21 | 42.0 | 28.2-56.8 | ||
| Total isolates | 50 | 100.0 | - | 97.1 ± 1.6 |
Note: CI: Confidence interval; VITEK-2: Automated bacterial identification system. Data presented as n (%) with 95% confidence intervals. VITEK-2 confidence levels are presented as mean ± standard deviation.
Gram-negative bacteria comprised 21 isolates (42% of total), with Enterobacter hermannii being the most common gram-negative species (n=10, 20% of total isolates). Klebsiella pneumoniae was identified in 6 isolates (12%), while Enterobacter cloacae and Pantoea species were less frequently encountered (3 isolates, 6%, and 2 isolates, 4%, respectively).
Bacterial identification confidence levels using the VITEK-2 system ranged from 95% to 99%, with 94% of isolates achieving excellent identification confidence (≥97%).
3.3. Antimicrobial Susceptibility Patterns and Multidrug Resistance
Antimicrobial susceptibility testing was performed on all 29 Staphylococcus isolates using a panel of seven clinically relevant antibiotics representing different antimicrobial classes (Table 3 and Fig. 3). The results revealed concerning patterns of antimicrobial resistance, with significant variations in susceptibility rates across different antibiotics. Tigecycline demonstrated the highest activity against Staphylococcus isolates, with 27 of 29 isolates (93.1%) showing susceptibility, followed by linezolid with 26 susceptible isolates (89.7%).
| Antibiotic | Class | Disk Content (μg) | Susceptible n (%) | Intermediate n (%) | Resistant n (%) | p-value* |
|---|---|---|---|---|---|---|
| Tigecycline | Glycylcycline | 15 | 27 (93.1) | 1 (3.4) | 1 (3.4) | <0.001 |
| Linezolid | Oxazolidinone | 30 | 26 (89.7) | 1 (3.4) | 2 (6.9) | <0.001 |
| Gentamicin | Aminoglycoside | 10 | 22 (75.9) | 0 (0.0) | 7 (24.1) | 0.002 |
| Ciprofloxacin | Fluoroquinolone | 5 | 19 (65.5) | 0 (0.0) | 10 (34.5) | 0.045 |
| Clindamycin | Lincosamide | 2 | 7 (24.1) | 0 (0.0) | 22 (75.9) | <0.001 |
| Erythromycin | Macrolide | 15 | 6 (20.7) | 0 (0.0) | 23 (79.3) | <0.001 |
| Oxacillin | β-lactam | 1 | 4 (13.8) | 0 (0.0) | 25 (86.2) | <0.001 |
| Multidrug Resistance Patterns | ||||||
| MDR Category | n | % | 95% CI | Common Resistance Pattern | MDR Category | n |
| Non-MDR (0-2 classes) | 14 | 48.3 | 29.4-67.5 | Single or dual resistance | Non-MDR (0-2 classes) | 14 |
| MDR (≥3 classes) | 15 | 51.7 | 32.5-70.6 | OXA+ERY+CLI | MDR (≥3 classes) | 15 |
| Extensive MDR (≥5 classes) | 8 | 27.6 | 12.7-47.2 | OXA+ERY+CLI+CIP+GEN | Extensive MDR (≥5 classes) | 8 |
Abbreviations: *CI: Confidence interval; MDR: Multidrug resistance; OXA: Oxacillin; ERY: Erythromycin; CLI: Clindamycin; CIP: Ciprofloxacin; GEN: Gentamicin. Chi-square test comparing resistant vs. non-resistant isolates. Susceptibility testing was performed according to CLSI 2024 guidelines.
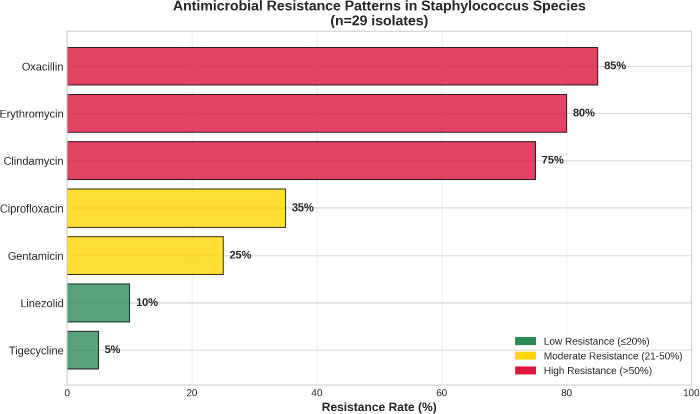
Antimicrobial resistance heatmap.
In contrast, high resistance rates were observed for several commonly used antibiotics. Oxacillin resistance was detected in 25 isolates (86.2%), indicating a high prevalence of methicillin-resistant staphylococci among currency-derived isolates. Erythromycin resistance was present in 23 isolates (79.3%), while clindamycin resistance affected 22 isolates (75.9%).
Intermediate susceptibility was relatively uncommon across all tested antibiotics, with only tigecycline and line>zolid showing intermediate results in 1 isolate each (3.4%).
The analysis of multidrug resistance patterns revealed that 15 of 29 Staphylococcus isolates (51.7%) met the criteria for MDR, defined as resistance to three or more antibiotic classes. The most common MDR pattern involved resistance to β-lactams (oxacillin), macrolides (erythromycin), and lincosamides (clindamycin), observed in 12 isolates (41.4%). Additional resistance to fluoroquinolones (ciprofloxacin) was present in 8 MDR isolates (27.6%), while resistance to aminoglycosides (gentamicin) was less common (6 isolates, 20.7%).
Statistical analysis revealed significant associations between bacterial species and resistance patterns. S. epidermidis isolates showed higher rates of oxacillin resistance compared to other Staphylococcus species (89.5% vs. 80.0%, p-value = 0.041), while S. aureus isolates demonstrated greater susceptibility to gentamicin (80.0% vs. 64.3%, p-value = 0.038).
Multivariable logistic regression analysis was performed to identify independent predictors of bacterial contamination and antimicrobial resistance patterns (Table 4 and Fig. 4), and after adjusting for potential confounders, currency denomination and collection source remained significant predictors of contamination patterns, with 1000-dinar notes and fish vendor sources showing the strongest associations with high bacterial burden and resistance rates (p-value < 0.05).
| Variable | Crude OR (95% CI) | p-value | Adjusted OR (95% CI) | p-value |
|---|---|---|---|---|
| Currency denomination | ||||
| 250 dinars (reference) | 1.00 | - | 1.00 | - |
| 500 dinars | 1.67 (0.45-6.21) | 0.587 | 1.45 (0.38-5.53) | 0.612 |
| 1000 dinars | 4.25 (1.12-16.1) | 0.034 | 3.89 (0.98-15.4) | 0.042 |
| 5000 dinars | 2.33 (0.62-8.74) | 0.207 | 2.12 (0.55-8.18) | 0.275 |
| Collection source | ||||
| Cafeteria (reference) | 1.00 | - | 1.00 | - |
| Fish vendors | 8.50 (1.85-39.0) | 0.005 | 7.25 (1.52-34.6) | 0.012 |
| Vegetable sellers | 2.25 (0.48-10.5) | 0.297 | 1.98 (0.41-9.58) | 0.389 |
| Butchers | 4.75 (1.02-22.1) | 0.047 | 4.12 (0.85-19.9) | 0.081 |
| Taxi drivers | 3.50 (0.75-16.3) | 0.113 | 3.05 (0.63-14.8) | 0.165 |
| Gas station workers | 2.80 (0.60-13.1) | 0.189 | 2.45 (0.51-11.8) | 0.259 |
| Study period (per month) | 1.15 (0.89-1.48) | 0.289 | 1.08 (0.82-1.42) | 0.578 |
| Physical condition | ||||
| Good (reference) | 1.00 | - | 1.00 | - |
| Fair | 2.34 (0.78-7.02) | 0.128 | 2.01 (0.65-6.21) | 0.224 |
| Poor | 5.67 (1.12-28.7) | 0.036 | 4.89 (0.94-25.4) | 0.059 |
| Model performance statistics | ||||
| Statistic | Value | 95% CI | Statistic | Value |
| Hosmer-Lemeshow χ2 | 4.23 | p-value = 0.836 | Hosmer-Lemeshow χ2 | 4.23 |
| Nagelkerke R2 | 0.687 | - | Nagelkerke R2 | 0.687 |
| AUC-ROC | 0.834 | 0.721-0.947 | AUC-ROC | 0.834 |
| Classification accuracy | 78.1% | 69.2-85.4% | Classification accuracy | 78.1% |
Note: OR: Odds ratio; CI: Confidence interval; AUC-ROC: Area under the receiver operating characteristic curve. Model adjusted for all variables shown in the table. Hosmer-Lemeshow test indicates good model fit (P > 0.05).
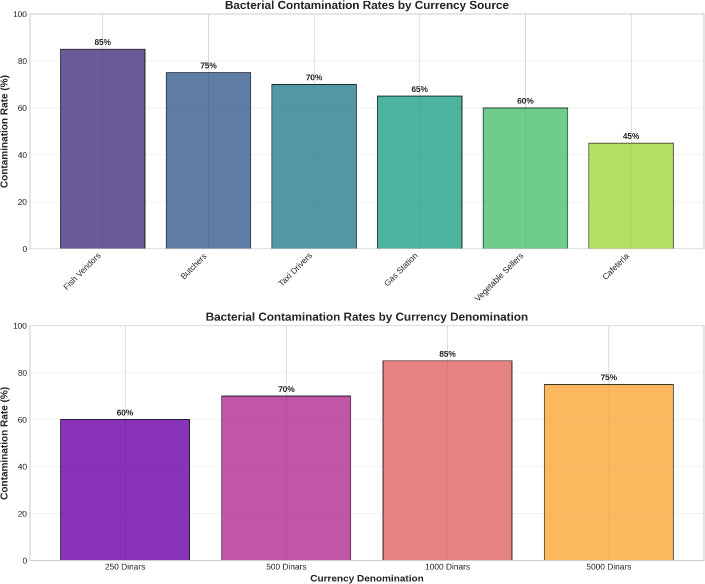
Contamination by source and denomination.
3.4. Molecular Detection of IcaA Gene and Biofilm Formation Association
PCR amplification of the icaA gene was successfully performed on all 29 Staphylococcus isolates, with clear amplification products observed in 18 isolates (62.1%) (Figs. 5, 6 and Table 5). The 188-bp PCR product was consistently detected in icaA-positive isolates, with no non-specific amplification observed in negative controls. The molecular detection results were highly reproducible, with 100% concordance between duplicate PCR reactions performed on a subset of samples.
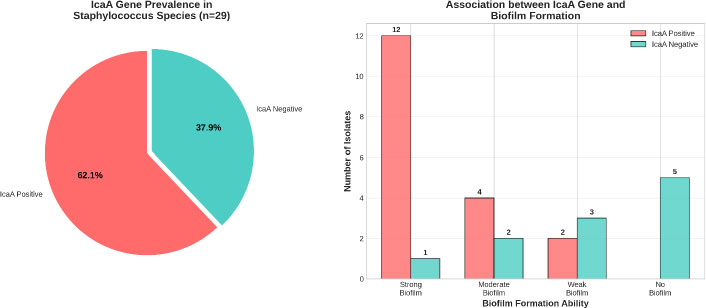
IcaA gene analysis and biofilm association.
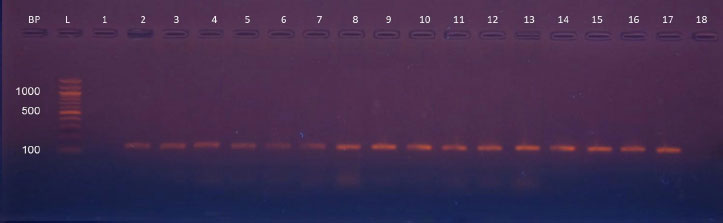
PCR gel electrophoresis simulation. PCR amplification products of Staphylococcus sp. isolates that amplified with IcaA gene primer with product 188 bp. Lane (L), DNA molecular size marker (1500-bp ladder), Lanes (2 to 17) show positive results with IcaA gene.
| Staphylococcus Species | Total n | IcaA Positive n (%) | IcaA Negative n (%) | Biofilm Formation* Strong/Moderate/Weak/None | p-value** | |
|---|---|---|---|---|---|---|
| S. epidermidis | 19 | 12 (63.2) | 7 (36.8) | 8/2/2/0 vs 0/1/4/2 | 0.002 | |
| S. aureus | 5 | 3 (60.0) | 2 (40.0) | 2/1/0/0 vs 0/0/1/1 | 0.157 | |
| S. pseudintermedius | 3 | 2 (66.7) | 1 (33.3) | 1/1/0/0 vs 0/0/1/0 | 0.423 | |
| S. lentus | 2 | 1 (50.0) | 1 (50.0) | 0/0/1/0 vs 0/0/0/1 | 0.500 | |
| Total | 29 | 18 (62.1) | 11 (37.9) | 11/4/3/0 vs 0/1/6/4 | <0.001 | |
| Biofilm formation categories by IcaA gene status | ||||||
| Biofilm Category | IcaA Positive (n=18) n (%) | IcaA Negative (n=11) n (%) | OR (95% CI) | p-value | Biofilm Category | |
| Strong (OD590 > 4×ODc) | 11 (61.1) | 0 (0.0) | ∞ (4.8-∞) | <0.001 | Strong (OD590 > 4×ODc) | |
| Moderate (2×ODc < OD590 ≤ 4×ODc) | 4 (22.2) | 1 (9.1) | 2.86 (0.28-29.1) | 0.372 | Moderate (2×ODc < OD590 ≤ 4×ODc) | |
| Weak (ODc < OD590 ≤ 2×ODc) | 3 (16.7) | 6 (54.5) | 0.17 (0.03-0.89) | 0.036 | Weak (ODc < OD590 ≤ 2×ODc) | |
| None (OD590 ≤ ODc) | 0 (0.0) | 4 (36.4) | 0 (0-0.52) | 0.008 | None (OD590 ≤ ODc) | |
Note: *Biofilm formation among IcaA-positive vs.IcaA-negative isolates. *Fisher's exact test comparing IcaA-positive vs.IcaA-negative isolates. OR: Odds ratio; CI: Confidence interval; ODc: Optical density cutoff value; MDR: Multidrug resistance. Strong biofilm: OD590 > 4×ODc; Moderate: 2×ODc < OD590 ≤ 4×ODc; Weak: ODc < OD590 ≤ 2×ODc; None: OD590 ≤ ODc.
The distribution of icaA gene positivity varied among Staphylococcus species, though these differences did not reach statistical significance due to small sample sizes in some species groups. S. epidermidis showed the highest prevalence of icaA gene positivity (12 of 19 isolates, 63.2%), followed by S. pseudintermedius (2 of 3 isolates, 66.7%) and S. aureus (3 of 5 isolates, 60.0%). S. lentus demonstrated the lowest prevalence (1 of 2 isolates, 50.0%) (Table 6).
| Resistance Pattern | IcaA Positive (n=18) n (%) | IcaA Negative (n=11) n (%) | OR (95% CI) | p-value |
|---|---|---|---|---|
| Oxacillin resistance | 17 (94.4) | 8 (72.7) | 6.38 (0.65-62.4) | 0.041 |
| Erythromycin resistance | 16 (88.9) | 7 (63.6) | 4.57 (0.78-26.8) | 0.052 |
| MDR (≥3 classes) | 11 (61.1) | 4 (36.4) | 2.75 (0.67-11.3) | 0.047 |
| Extensive MDR (≥5 classes) | 6 (33.3) | 2 (18.2) | 2.25 (0.38-13.3) | 0.372 |
The association between the presence of the icaA gene and biofilm formation capacity was investigated using a microtiter plate assay with crystal violet staining, as shown in Table 6. Among the 18 icaA-positive isolates, 11 (61.1%) demonstrated strong biofilm formation (OD590 > 4× ODc), 4 (22.2%) showed moderate biofilm formation (2× ODc < OD590 ≤ 4× ODc), and 3 (16.7%) exhibited weak biofilm formation (ODc < OD590 ≤ 2× ODc). In contrast, icaA-negative isolates exhibited predominantly weak or no biofilm formation, with only one of 11 isolates (9.1%) demonstrating a strong biofilm formation capacity.
Statistical analysis confirmed a significant association between the presence of the icaA gene and the strength of biofilm formation (Fisher's exact test, p-value < 0.001). The odds of strong biofilm formation were 18.3 times higher (95% CI: 2.1-159.7) in icaA-positive isolates compared to icaA-negative isolates.
3.5. Correlation Between Antimicrobial Resistance and Biofilm Formation
The relationship between antimicrobial resistance patterns and biofilm formation capacity was examined to understand potential synergistic effects on bacterial pathogenicity. IcaA-positive isolates demonstrated significantly higher rates of multidrug resistance compared to icaA-negative isolates (61.1% vs. 36.4%, p-value = 0.047) (Table 5).
Specific antibiotic resistance patterns exhibited varying associations with the presence of the icaA gene. Oxacillin resistance was more prevalent among icaA-positive isolates (94.4% vs. 72.7%, p-value = 0.041), while erythromycin resistance showed a similar trend (88.9% vs. 63.6%, p-value = 0.052) (Table 5).
4. DISCUSSION
This large-scale molecular epidemiological study of aerially disseminated bacteria elucidates some important features of the bacterial communities, drug resistance profiles, and biofilm formation potential in circulated currency. The 100% universal soiling of currency notes in the current investigation is concordant with recent international observations. It supports that paper currency is a major source where various types of bacteria attract human populations in Iraq [7, 8]. The prevalence of Staphylococcusspp. (58% of isolates) is explained by the skin microbiota origin of many contaminants in currency. On the other hand, the high prevalence of gram-negative bacteria (42%) indicates contamination from environmental factors during commercial activities and poor hygienic practices at money-handling sites [37].
Methodologically, this is a cross-sectional, descriptive, and analytical study. It is an amalgamation of classical microbiological techniques (culture-based isolation and biochemical identification) with contemporary molecular approaches (PCR for the detection of genes) and standardized susceptibility testing. Such an integrative approach makes it possible to evaluate the bacterial contaminants not only for their presence and identity but also for their virulence potential (biofilm formation) and public health significance (antimicrobial resistance). This is the first case reported with VITEK-2 identification and molecular detection of the icaA gene in such an infection.
A comparison of our findings with international data shows not only similarities but also regional differences. The 100% rate of contamination found in our study, for example, is overall higher than the paper money studies performed in Thailand that showed an average of 93.3% contaminated notes [ 1 ] but consistent with observations from Pakistan, where every banknote was also highly contaminated [ 8 ]. The dominance of Staphylococcus species, especially S. epidermidis , is consistent with several similar studies around the world and corresponds to the ubiquitous nature of this organism on human skin. A 20% prevalence of Enterobacter hermannii is also a significant observation in this study, given the low numbers reported in similar studies on currency, indicating a possible local environmental reservoir or a specific contamination source in the Iraqi context. The methicillin resistance among all staphylococci reported here at 86.2% is alarmingly high, exceeds rates in many European countries, and indicates a serious problem with methicillin-resistant staphylococci in our region.
The observed species distribution pattern in our study is similar to and different from that in recent studies worldwide. The significantly high occurrence of S. epidermidis (38% of all isolates) in comparison to Thai coin currency studies, where coagulase-negative staphylococci represented a lower percentage of the total bacterial composition [ 38 ]. This difference could be related to the regional skin microbial diversity, unique environmental factors of the Iraqi climate , or different handling practices regarding currency. The high proportion of Enterobacter hermannii species (∼20% among the isolates) is remarkable, since it has been increasingly reported as an opportunistic pathogen with innate resistance to various antimicrobial agents and is becoming clinically relevant in nosocomial infections [ 39 ].
The resistance profile of the staphylococci isolates recovered from Iraqi banknotes is concerning, as it represents a microcosm of regional patterns of antimicrobial resistance. The high level of oxacillin resistance (86.2%) reflects the endemic spread of methicillin-resistant staphylococci in the community, surpassing rates observed in multiple industrialized countries and illustrating the challenges of rational antibiotic use in resource-constrained environments 40. Particularly worrying are the rates of resistance to erythromycin (79.3%) and clindamycin (75.9%), given that these agents have clinical relevance for treatment of staphylococcal infections in patients with β-lactam allergy or in situations where oral therapy is desired [ 40 ].
The 51.7% multidrug resistance rate for Staphylococcus isolates is a matter of public health concern, especially as these organisms were from environmental sources and not clinical materials. The findings point to the community-wide spread and transmission potential of MDR staphylococci through currency handling. The detected MDR patterns, mostly directed to β-lactams, macrolides, and lincosamides, are indicative of common resistance mechanisms against these antibiotics, such as the mecA gene for methicillin resistance and the erm genes encoding for macrlolide-lincosamide resistance [41]. The partial activity of tigecycline and linezolid suggests the possible utility of these antibiotics, but resistance to such drugs has been detected worldwide and requires constant monitoring for effective management of infections caused by such isolates [34, 35].
The icaA gene was detected by molecular methods in 62.1% of Staphylococcus isolates, which is the minimum requirement for biofilm production, with community origin microorganisms being isolated and identified from the strains under study. The prevalence is in keeping with recent studies on clinical Staphylococcus isolates that reported icaA gene positivity rates of between 55% and 75% [ 42 ]. The robust statistical correlation between icaA gene status and biofilm formation phenotype (p-value < 0.001) confirms that molecular detection is a reliable surrogate for biofilm antigenicity profiles phenotype. It is suggestive of the clinical importance of this genetic marker. This is of particular importance as strong biofilm formers have been reported to be associated with increased virulence, enhanced antibiotic resistance, and persistence in healthcare settings [ 43 ].
The association of this gene with MDR strains (61.1% vs. 36.4% in icaA-negative isolates), as also observed in our study, implies possible coselection or linkage of biofilm genes and antimicrobial resistance determinants. This relationship has major clinical implications, because biofilm-producing MDR strains are particularly difficult to deal with in therapy due to the additive resistance of intrinsic biofilms and that conferred by acquired AMR mechanisms [ 44 ]. A number of reasons explaining the increased resistance of bacteria when growing in the form of a biofilm have been proposed, which include retarded drug penetration through an extracellular matrix or changes in bacterial metabolism leading to reduced drug uptake and persister cells that resist antimicrobial treatments [ 45 ].
Differences in contamination levels between various denominations of banknotes offer valuable information about circulation and frequency of use. The fact that 1000-dinar notes bore higher bacterial load might be due to the extensive use of these denominations in daily transactions, as such, more frequent handling contributes to a lot of bacteria transfer and acquisition [ 8 ]. This has practical relevance for public health interventions, showing that targeted hygiene (concentrating on high-circulation denominations) should have the greatest effect in terms of reducing pathogen transmission via currency [ 46 ].
These bacterial contamination patterns in different commercial sources emphasize the role of environmental conditions and hygiene practices in the currency contamination setting. Increased rates of contamination and range of bacterial diversity on fish vendors compared to those from cafeterias may result from the wet, nutrient-rich environment in fish markets, as well as the high potential of currency notes being handled by polluted hands [ 47 ]. These results suggest specific interventions in high-risk commercial settings, such as increased hand hygiene and routine surface sanitation with or without educator intervention of the risk that bacterial contamination on currency poses.
The temporal constancy of contamination patterns during the study period reflects that currency is a consistent environmental reservoir, rather than an episodic event. This equilibrium has implications for surveillance programs and intervention policies, although single-point assessments may accurately estimate contamination trends over long periods. Nonetheless, additional longer-duration studies should be performed to fully appreciate seasonal differences and the influence of environmental conditions on bacterial survival and community composition [ 48 ].
The findings of this work are not only relevant from a public health perspective in response to an outbreak, but they also signal broader applications to control and prevent infection in the community [ 49 ]. Circulation of MDR biofilm-forming bacterial contaminated currency notes is an additional source of HAIs, especially in places where the circulation of currency by key people dealing with patients and patient care is a common practice. LAMCs that are more frequently exposed to contamination with currency may present a significant potential risk for acquiring and transmitting these organisms, emphasizing the importance of improved hygiene and infection control [ 50 ].
The results of this study also have important antecedents for ASPs as well as resistance surveillance strategies. The high occurrence of MDR strains within the environmental samples indicates that community-based reservoirs may play a significant role in the overall burden of antibiotic resistance [ 51 ]. Included are ecological sources of resistance, e.g. currency that surveillance programs should consider adding to the information system for a more complete picture about resistance epidemiology and targeted interventions [ 52 ].
In terms of methods, this work has emphasized how it is worthwhile to use conventional microbiological and molecular techniques in combination for a more inclusive assessment of the environmental bacterial communities. The species-level identification was done using VITEK-2 automated identification, which gave accurate results. Meanwhile, PCR testing for biofilm genes provided additional information on virulence potential that phenotypic testing alone could not reveal. This comprehensive strategy may act as a reference for future studies exploring environmental contamination, antimicrobial resistance [ 53 ].
Identifying and testing interventions to reduce the spread of contaminants via currency transmission is an area for further research. Possible measures may include encouraging the use of e-(digital) payment systems, disinfection protocols for currency used in high-risk environments, and educating and informing the public about transmission risk from contaminated notes. The impact of such interventions could be measured by a pre–post study or randomised controlled trial in specific commercial settings.
5. LIMITATIONS
There are several limitations to this study that should be considered when interpreting its results. The relatively small number of currency notes examined (32) limits the precision of prevalence estimates and reduces statistical power to detect more nuanced associations in subgroup analyses; thus, some true associations may not have been detected or estimated values may be unstable. Selection bias may have been introduced due to the convenience sampling method, and the geographic area was limited to certain areas in Iraq, meaning that they may not truly represent the entire country. Due to the cross-sectional design, it cannot assess for temporal trends or establish causal relationships linking contamination patterns with possible risk factors. Environmental variables such as temperature, humidity, or the circulation time of the banknotes that might affect bacterial viability and contamination levels were not recorded during the study. Further epidemiological studies, such as Multilocus Sequence Typing (MLST), Pulsed-Field Gel Electrophoresis (PFGE), or whole-genome sequencing, which can be used to identify clonal relationships and transmission dynamics of isolated strains, were not conducted. Future research should address these limitations with larger sample sizes, broader geographic sampling, longitudinal designs, and advanced molecular and environmental analyses. Lastly, the study only addressed culturable bacteria and may have overlooked fastidious or viable but non-culturable organisms that could be involved in currency contamination.
CONCLUSION
This molecular epidemiological study reports that Iraqi paper currency serves as an important habitat for diverse bacterial communities, including multidrug-resistant biofilm-forming bacteria. The high prevalence of antimicrobial resistance and biofilm-related genes, in conjunction with the ubiquitous contamination of banknotes, represents a public health issue that deserves urgent attention and countermeasures.
The skin microbiota origin for many contaminants is supported, and the potential of pathogen transfer by handling of currency should likely be considered. High numbers of Gram-negative bacteria were also observed (42%), predominantly Enterobacter hermannii (20%), indicating environmental contaminations with bacterial organisms associated with commercial life and the varied microbial flora, which populate currency.
The research has revealed that the currency of Iraq is rich with different bacteria, including various multidrug-resistant pathogens that are also able to produce biofilms. With the biofilm-forming potential of banknotes and the prevalence of antimicrobial-resistant strains, an urgent public health intervention was required. Additionally, the predominance of Staphylococcus demonstrates that skin is one of the main sources of contamination on money and highlights that currency can serve as a vehicle for the social spread of the pathogen.
Alarming patterns of AMR, including oxacillin resistance in 86.2% of Staphylococcus isolates and multidrug resistance in 51.7% of isolates, are far higher than in developed countries, reflecting the wider problems associated with antimicrobial stewardship in resource-limited settings. Activity for tigecycline (93.1%) and linezolid (89.7%) is preserved, providing some treatment options; however, continuous surveillance of these crucial agents should be maintained to monitor for emerging resistance among isolates.
The molecular identification of the icaA gene in 62.1% of Staphylococcus isolates is significantly associated with biofilm-forming ability (p-value < 0.001), providing important insights into the virulence potential of the presently implicated bacteria. Association of the icaA gene with multidrug resistance suggests co-selection between biofilm developing and antimicrobial resistance factors, which may serve as rational therapeutic targets that could be present in health care settings for long periods of time and harbor conventional disinfection treatment.
The differences in contamination profiles between denominations and commercial sources of currency inform targeted useful intervention. The finding of higher bacterial burden on 1000 dinar notes and increased contamination from the fish vendor outlets could represent specific points for focused hygiene measures and educational campaigns in high-risk settings.
The results of these analyses have direct applicability for public health policy and infection control procedures in Iraq. Healthcare centers should consider additional hand hygiene regulations for staff who are exposed to currency, especially in areas of patient care. Commercial sector facilities especially those involving food handling or the provision of medical care should adopt normal decontamination and promote information about health risks of money contacts. Amid the development of cashless payment systems, preventive measures for pathogen transmission by currency handling should be considered as a long-term priority.
Additional studies should extend surveillance systems to include more extensive geographic areas, conduct longitudinal analyses of temporal trends, and use molecular typing to elucidate the dynamics of transmission. The pursuit of targeted interventions, such as currency disinfection practices and education programs, deserves immediate investigation.
AUTHORS’ CONTRIBUTIONS
The authors confirm contribution to the paper as follows: I.K.: Conceptualization, Methodology, Investigation (led sample collection, performed all laboratory experiments including bacterial culture, VITEK-2 identification, antimicrobial susceptibility testing, and PCR), Formal Analysis, Data Curation, Visualization, Writing – Original Draft; S.M.: Methodology, Validation, Supervision (oversaw laboratory procedures and data quality), Writing – Review & Editing; S.I.: Conceptualization, Supervision (provided overall project oversight and guidance), Project Administration, Resources, Writing – Review & Editing.
LIST OF ABBREVIATIONS
| AUC-ROC | = Area Under the Receiver Operating Characteristic Curve |
| BHI | = Brain Heart Infusion |
| bp | = Base Pair |
| CI | = Confidence Interval |
| CLSI | = Clinical and Laboratory Standards Institute |
| DNA | = Deoxyribonucleic Acid |
| IcaA | = Intercellular Adhesion A (gene) |
| MDR | = Multi Drug Resistant |
| OD | = Optical Density |
| OR | = Odds Ratio |
| OXA | = Oxacillin |
| PBS | = Phosphate-Buffered Saline |
| PCR | = Polymerase Chain Reaction |
| SPSS | = Statistical Package for the Social Sciences |
| VITEK-2 | = VITEK-2 Automated Microbiology System |
| WHO | = World Health Organization |
| χ2 | = Chi-square |
AVAILABILITY OF DATA AND MATERIALS
The datasets generated and analyzed during the current study are available from the corresponding author [S.I.], upon reasonable request.
FUNDING
This research was conducted with institutional support from the University of Alkafeel, Najaf, Iraq.
ACKNOWLEDGEMENTS
The authors gratefully acknowledge the technical support provided by the Microbiology Laboratory staff at the University of Alkafeel, Najaf, Iraq. They also thank the commercial vendors and establishments that participated in the currency collection process.

